
What is coronary artery disease (CAD)?
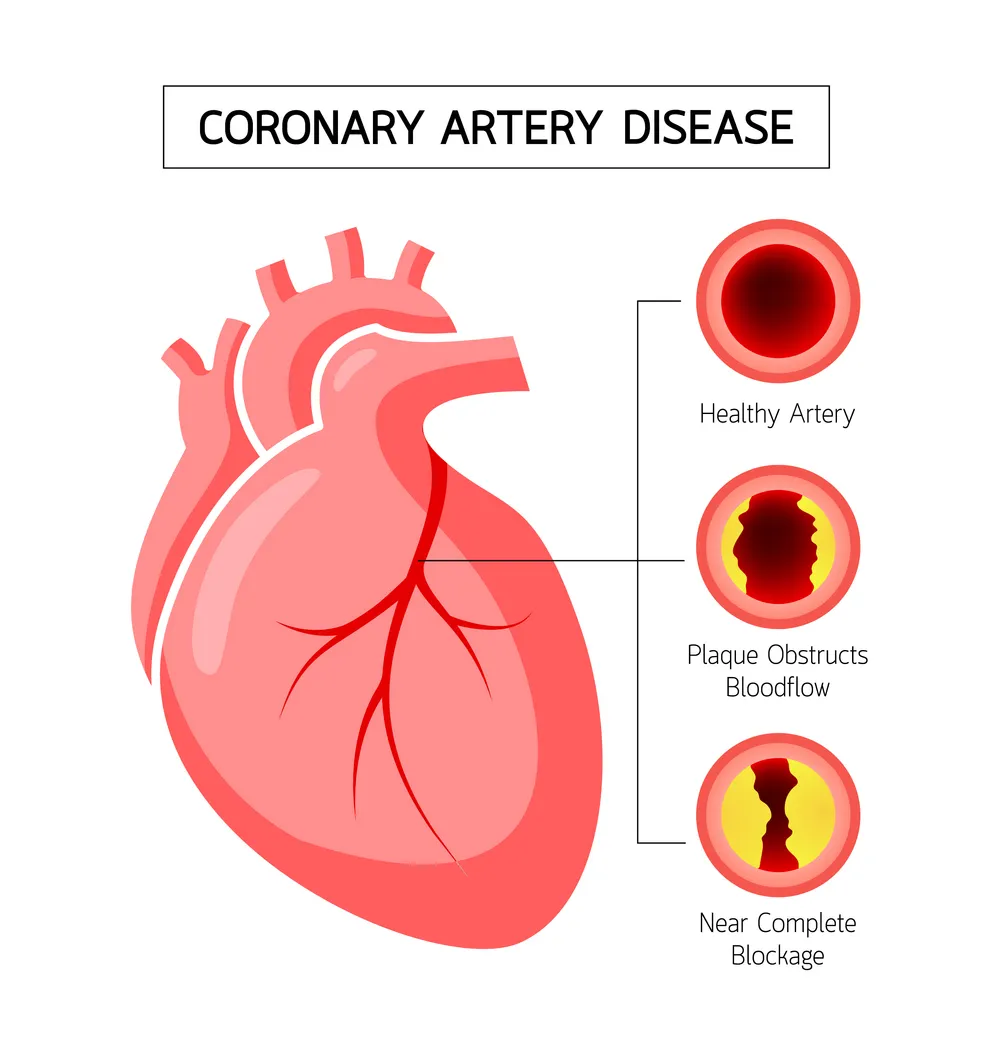
Coronary artery disease (CAD) is a condition whereby the blood vessels supplying the heart, known as the coronary arteries, become narrowed or blocked by the build-up of fatty plaques.
These fatty plaques prevent the delivery of oxygen and nutrients to the heart muscle, which can damage heart tissue. When blood flow to regions of heart tissue becomes temporarily reduced, this can cause chest pain – a condition known as angina.
Fatty plaques inside coronary arteries can also suddenly rupture and form a blood clot. This cuts off blood flow to a region of heart tissue, causing it to be starved of oxygen. This is what happens in a heart attack (myocardial infarction).
Coronary artery disease (CAD) greatly increases the risk of having a heart attack, and CAD (also known as coronary heart disease (CHD) or ischaemic heart disease (IHD)) is thought to be responsible for approximately 1 in 4 deaths in the USA each year.
Our lifestyle has a significant impact on our risk of CAD. Smoking, physical inactivity, alcohol use, and unhealthy diets that cause high blood levels of sugar (glucose) and lipids (fat and cholesterol), are all known to increase the risk of developing CAD.
By contrast, exercise, a healthy diet, giving up smoking, and reducing blood sugar and lipid levels can all help to prevent CAD.
KEY POINTS
- Coronary artery disease (CAD) is a condition in which fatty plaques build up in the arteries supplying the heart.
- This restricts blood flow to the heart tissue and increases the risk of having a heart attack.
What causes coronary artery disease (CAD)?
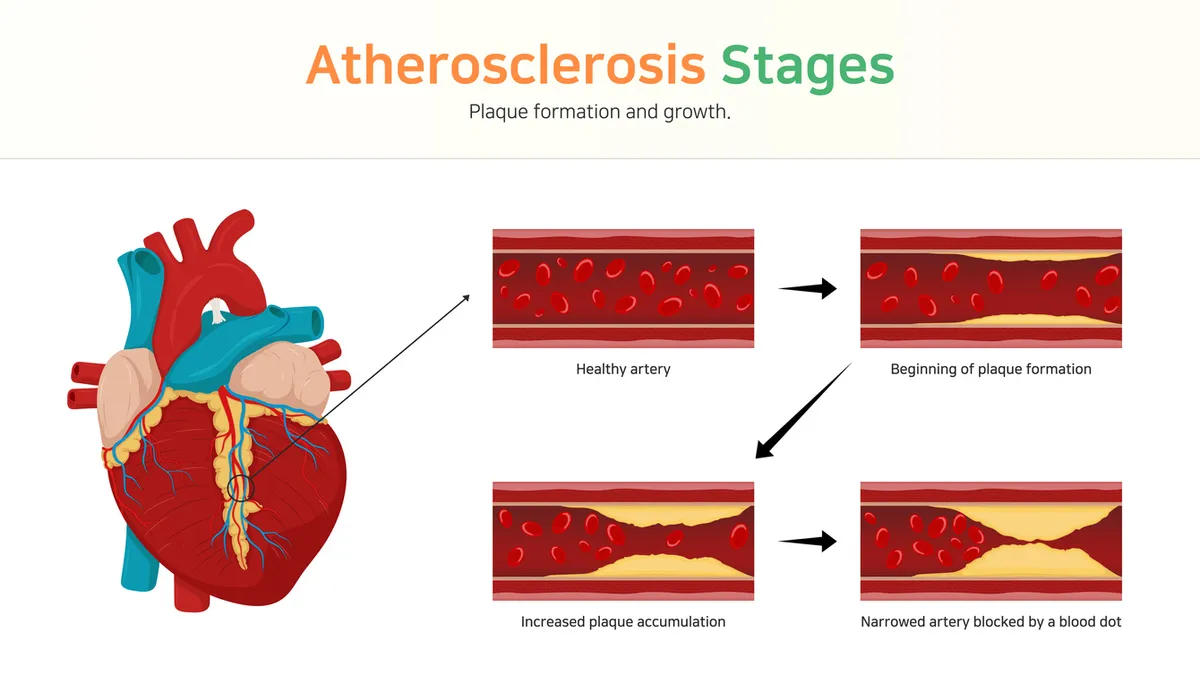
The underlying process in coronary artery disease (CAD) is atherosclerosis:- the build-up of fatty, cholesterol-rich plaques (known as atheromas) in the walls of arteries. In CAD, atheroma specifically builds up in the coronary arteries that supply the heart.
Atherosclerosis in more detail
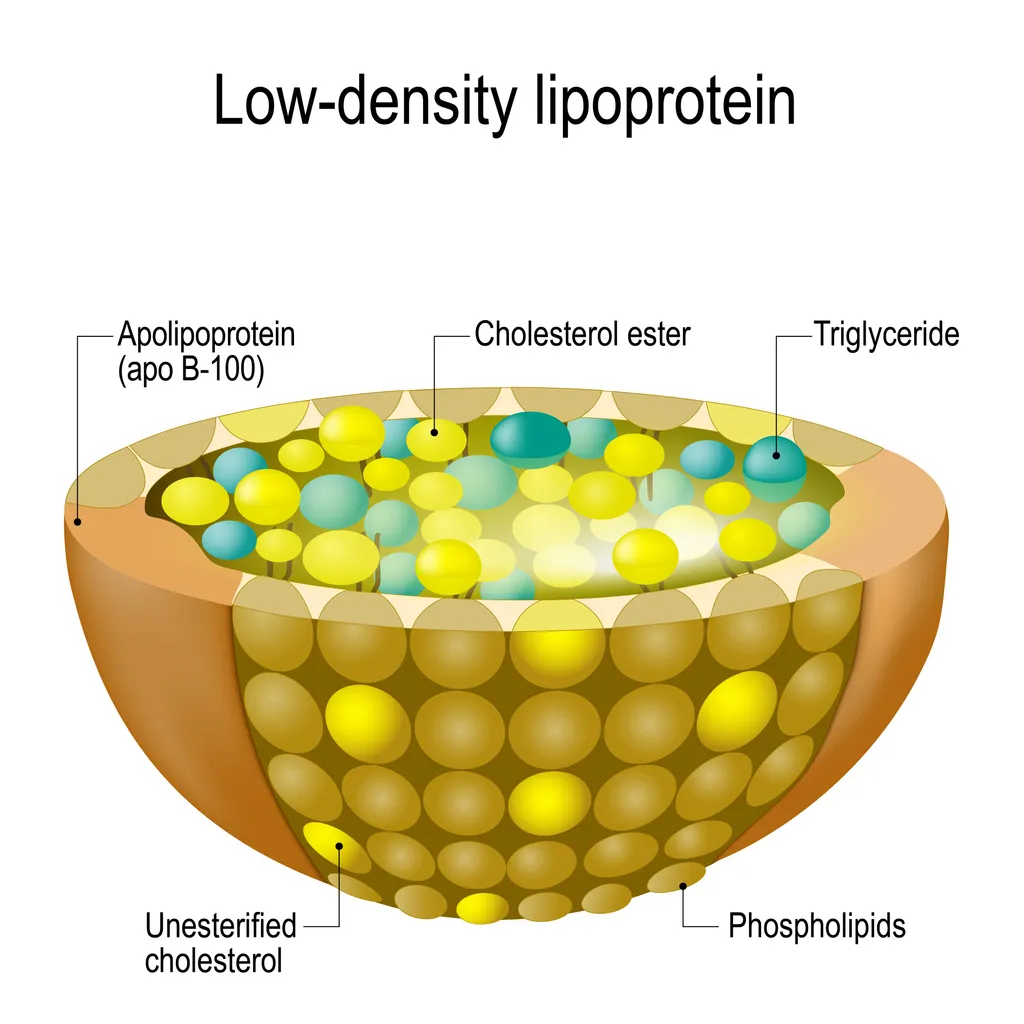
Cholesterol is a fat-like substance used to make cell membranes, hormones, and signalling molecules. It gets transported in the bloodstream in specialised particles known as lipoprotein particles.
In atherosclerosis, cholesterol in a particular type of lipoprotein particle (known as low-density lipoproteins (LDLs)) gets deposited into the lining of arteries, leading to the formation of fatty plaques. Cholesterol transported in these particles is known as LDL cholesterol.
The formation of a fatty plaque is a gradual process that takes several years, and occurs after initial damage to the inner lining of an artery (called the vascular endothelium). Many things can cause initial damage to your arterial lining, including physical injury from high blood pressure, toxins (e.g. such as those in cigarette smoke), and inflammation.
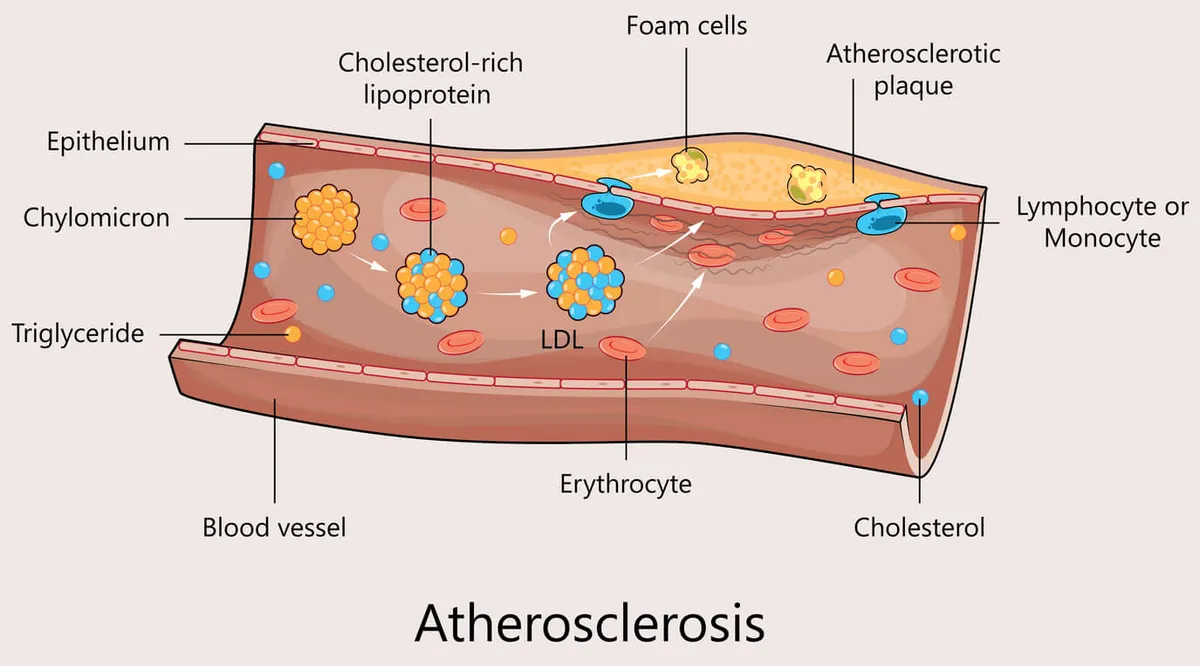
After initial damage to the arterial lining, cholesterol particles accumulate at the site of injury and undergo a chemical change known as oxidisation. Oxidised LDL cholesterol then triggers an inflammatory response, causing white blood cells called macrophages to arrive at the injury site.
Macrophages then take up the oxidised cholesterol, which gives them a yellowish, foamy appearance. For this reason, they are known as foam cells. Foam cells then die and accumulate in the arterial lining, forming a fatty streak.
As more foam cells accumulate, the fatty streak gradually enlarges into a fatty plaque. The plaque also becomes calcified, making it harder.
Source:Melaku, L., & Dabi, A. (2021). The cellular biology of atherosclerosis with atherosclerotic lesion classification and biomarkers. Bulletin of the National Research Centre, 45(1), 1-22.
After a long period (often years), the plaque may become unstable and eventually rupture. Rupture of a fatty plaque activates platelets and clotting factors in your bloodstream, causing the formation of a blood clot (thrombus) around the ruptured plaque. The blood clot may then completely occlude blood flow to the heart, causing a heart attack.
KEY POINTS
- Coronary artery disease (CAD) occurs due to the gradual build-up of fatty plaques in the lining of arteries - a process called atherosclerosis.
- Atherosclerosis involves damage and inflammation of arterial linings, which causes the deposition of cholesterol into fatty plaques.
- Smoking, high blood sugar levels, and chronic inflammation can all damage arterial linings and promote the development of fatty plaques.
- Fatty plaques can eventually rupture and form a blood clot that completely obstructs an artery. This is what happens in a heart attack.
What is LDL cholesterol (LDL-C)?
LDL cholesterol stands for low-density lipoprotein cholesterol (LDL-C).
It is sometimes called ‘bad’ cholesterol as it this type of cholesterol that gets deposited into fatty plaques.
As mentioned earlier, cholesterol is transported around the bloodstream in specialised particles called lipoproteins. Low-density lipoproteins, in particular, carry cholesterol to peripheral tissues, such as skeletal muscle, ovaries, testes, and liver. Cholesterol transported in these low-density particles is referred to as LDL-cholesterol.
(You can read more about the different types of lipoprotein particles and cholesterol in the Cholesterol and Ageing trait article).
High levels of cholesterol in LDL particles can also encourage the deposition of cholesterol into arterial linings, causing the formation of fatty plaques (atherosclerosis). As explained in the previous section, fatty plaques develop after intial injury to arterial linings. This triggers inflammation within the arterial wall, causing LDL cholesterol to be chemically modified into oxidised LDL-cholesterol. It is this oxidised LDL-cholesterol that gets taken up by white blood cells and incorporated into fatty plaques.
On this note, there is ample evidence to suggest that higher blood levels of LDL-C are linked to an increased risk of atherosclerosis and coronary artery disease (CAD).
KEY POINTS
- LDL cholesterol (LDL-C) stands for low-density lipoprotein cholesterol.
- LDL-C is sometimes known as 'bad' cholesterol.
- In atherosclerosis, LDL-C is chemically modified (oxidised) and deposited into fatty plaques.
- High levels of LDL-C increase the risk of atherosclerosis and coronary artery disease (CAD).
Why are high LDL cholesterol levels bad for us?
High levels of LDL cholesterol (LDL-C) circulating in our bloodstream can increase our risk of us damaging our arterial linings and forming fatty plaques in our arteries. In other words, high LDL-C levels promote atherosclerosis in arteries, including the coronary arteries supplying the heart.
In this respect, several studies show that higher levels of LDL-C are linked to a greater risk of coronary artery disease (CAD). For example, the graphs below are from the Cooper Center Longitudinal study in which 36,375 subjects, who were deemed low risk for developing atherosclerotic cardiovascular disease, were followed up for an average (median) of 26.8 years.
As you can see in the graphs, the incidence of deaths due to cardiovascular disease (CVD) and coronary artery (heart) disease (CHD) was greater in those with higher LDL-C levels. More specifically, a blood LDL-C level of above 160 mg/dL (or 4.1 mmol/L) was linked to a 50-70% increased risk of death due to cardiovascular disease after adjusting for age.
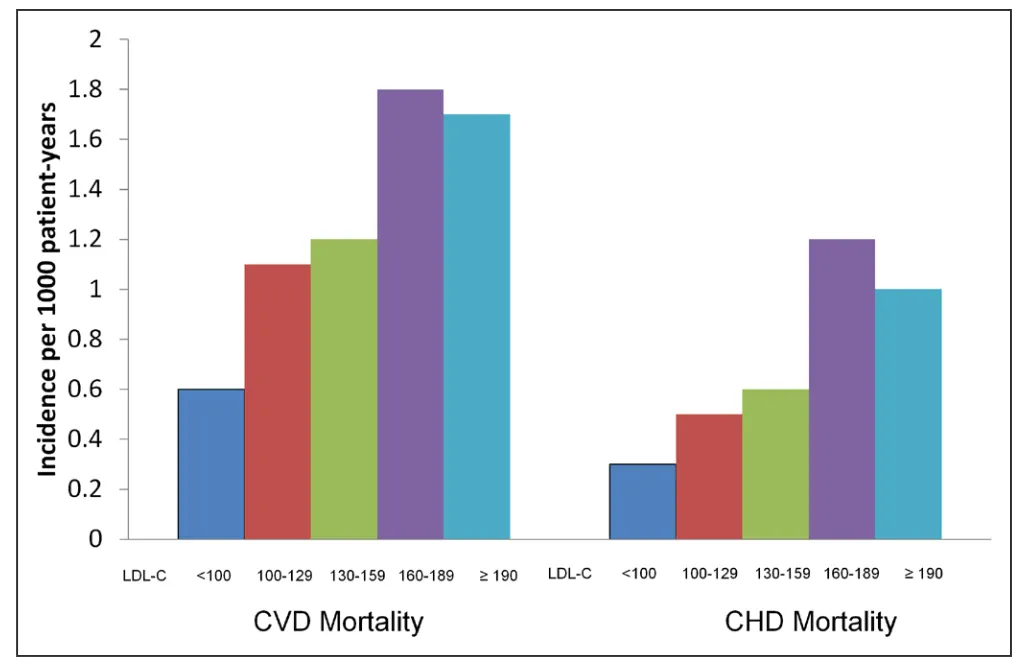
Source: Abdullah, S. M., Defina, L. F., Leonard, D., Barlow, C. E., Radford, N. B., Willis, B. L., ... & Khera, A. (2018). Long-term association of low-density lipoprotein cholesterol with cardiovascular mortality in individuals at low 10-year risk of atherosclerotic cardiovascular disease: results from the Cooper Center Longitudinal Study. Circulation, 138(21), 2315-2325.
Conversely, other studies have shown that reducing LDL-C levels, for example by using a class of drug known as statins, is associated with a decreased risk of cardiovascular disease (including coronary artery disease).
Analyses of various clinical trials have found that there appears to be a roughly linear relationship between lowering LDL-C levels and reduction in risk of cardiovascular events, such as heart attack and stroke. This is illustrated in the graph below.

Source: Kim, J., McEvoy, J. W., Nasir, K., Budoff, M. J., Arad, Y., Blumenthal, R. S., & Blaha, M. J. (2014). Critical review of high-sensitivity C-reactive protein and coronary artery calcium for the guidance of statin allocation: head-to-head comparison of the JUPITER and St. Francis Heart Trials. Circulation: Cardiovascular Quality and Outcomes, 7(2), 315-322.
Given this link between higher LDL-C levels and risk of cardiovascular disease, it is widely held that “lower is better” when it comes to optimal LDL cholesterol levels. In line with this, the NHS suggest a healthy blood LDL-C level is less than or equal to 3 mmol/L (116 mg/dL).
US guidelines suggest a healthy LDL-C level is less than 2.6 mmol/L (100 mg/dL) and even lower (<1.8mmol/L (70mg/dL)) for people who have coronary artery disease.
It is also worth pointing out that LDL cholesterol levels in isolation are not the only determinant of cardiovascular risk. We also have high-density lipoprotein (HDL) particles that transport cholesterol away from arterial linings and peripheral tissues to be removed or further metabolised by the liver.
Higher levels of HDL cholesterol, sometimes known as ‘good’ cholesterol, can protect against atherosclerosis and cardiovascular disease. The ratio of ‘bad’ LDL cholesterol and ‘good’ HDL cholesterol circulating in our bloodstream is therefore an important determinant of our overall cardiovascular risk.
KEY POINTS
- High LDL cholesterol levels increase the risk of cardiovascular diseases, including coronary artery disease (CAD).
- Reductions in LDL-C levels have been shown to reduce the risk of coronary artery disease.
- Generally speaking, when it comes to LDL-C levels and CAD risk: "the lower the better."
- A healthy LDL cholesterol level is considered to be <100 -116 mg/dL (<2.6 -3.0 mmol/L).
What is the PSRC1 gene?
The PSRC1 gene encodes a protein known as proline/serine rich coiled coil 1, which plays a role in cell division.
Interestingly, variants of the PSRC1 gene and the closely-related SORT1 (Sortilin 1) and CELSR2 (Cadherin EGF LAG Seven Pass Type Receptor 2) genes have been linked to cardiovascular disease.
On this note, a single nucleotide polymorphism (SNP) in the PSRC1 gene, designated rs599839, causes an A > G change in the DNA code, giving rise to two different PSRC1 variants or alleles: ‘A’ and ‘G’.
The ‘A’ allele has been associated with higher LDL-cholesterol levels and an increased risk of coronary artery disease (CAD).
KEY POINTS
- The PSRC1 gene, along with the closely related SORT1 and CELSR2 genes, has been implicated in coronary artery disease.
- The 'A' allele / variant (rs599839) of the PSRC1 gene has been associated with higher LDL cholesterol levels and increased coronary artery disease (CAD) risk.
How do variants of the PSRC1 gene affect LDL cholesterol levels?
The ‘A’ variant or allele (rs599839) of the PSRC1 gene has been associated with higher levels of LDL-cholesterol.
For example, a 2008 study, which pooled and analysed the data of roughly 15,000 people, found that each copy of the ‘A’ allele was associated with an approximately 0.15 mmol/L higher LDL-C level compared to those with the GG genotype.
The Ludwigshafen Risk and Cardiovascular Health Study reported similar findings.
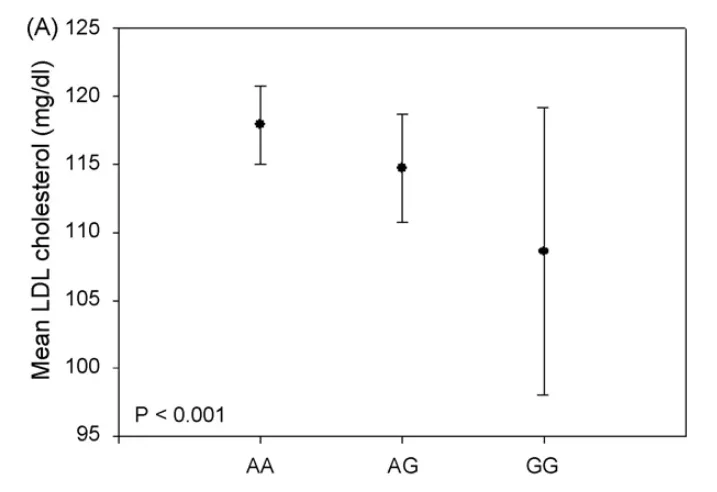
Source: Kleber, M. E., Renner, W., Grammer, T. B., Linsel-Nitschke, P., Boehm, B. O., Winkelmann, B. R., ... & März, W. (2010). Association of the single nucleotide polymorphism rs599839 in the vicinity of the sortilin 1 gene with LDL and triglyceride metabolism, coronary heart disease and myocardial infarction: the Ludwigshafen risk and cardiovascular Health study. Atherosclerosis, 209(2), 492-497.
As illustrated in the graph above, those with one (AG genotype) and two (AA genotype) copies of the ‘A’ allele had higher median LDL-C levels of 117.9 and 114.7 mg/dL, respectively. This was significantly higher than the LDL-C level for those with the GG genotype (108.6 mg/dL).
The reason why PSRC1 gene variants are associated with differences in LDL-C levels remains to be understood. It is possible that PSRC1 (as well as SORT1 and CELSR2) gene variants affect the metabolism of fat and cholesterol in lipoprotein particles.
KEY POINTS
- The 'A' allele (rs599839) of the PSRC1 gene is associated with higher LDL-cholesterol levels compared to the 'G' allele.
- 'A' allele carriers (particularly those with two copies - the AA genotype) are shown to have higher LDL-C levels.
- 'A' allele carriers are also shown to have higher total cholesterol and lower HDL-C levels.
How do variants of the PSRC1 gene affect risk of coronary artery disease (CAD)?
People who carry the ‘A’ allele (rs599839) of the PSRC1 gene are shown to have a higher risk of coronary artery disease (CAD).
A 2017 meta-analysis of genome-wide association studies, encompassing 18,108 subjects, found that people with the AA genotype had an 1.18 times higher odds of having CAD compared to those with the AG and GG genotypes. This is illustrated in the Forest plot below.
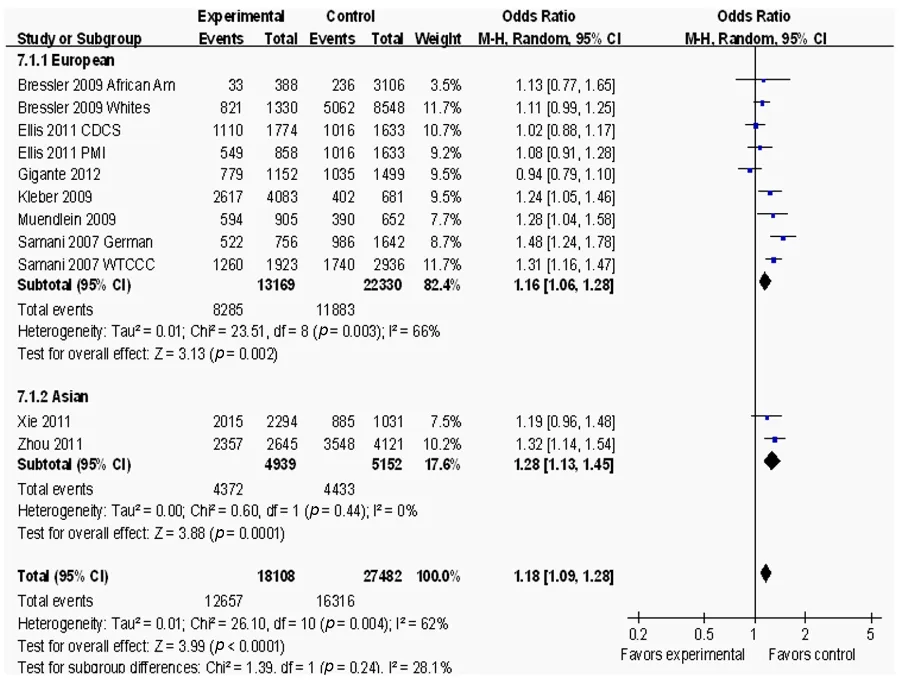
Source: He, Q. C., Hu, Y. Y., Zhang, Q. P., Tan, L. L., Liu, Y. H., Liu, T., ... & Liang, N. (2017). A meta-analysis of three identified single nucleotide polymorphisms at 1p13. 3 and 1q41 and their associations with lipid levels and coronary artery disease. The Kaohsiung Journal of Medical Sciences, 33(1), 1-10.
The effect of the ‘A’ allele of the PSRC1 gene on coronary artery disease (CAD) risk is likely mediated by its effects on LDL cholesterol levels.
As mentioned earlier, LDL-C promotes atherosclerosis and higher LDL-C levels are widely shown to increase the risk of CAD. Therefore, by raising LDL-C levels, the ‘A’ allele increases a person’s CAD risk.
In this respect, the same 2017 meta-analysis mentioned above found that those with the AA genotype also had significantly higher total and LDL cholesterol levels, but lower HDL cholesterol levels. Again, this is shown in the Forest plot below.
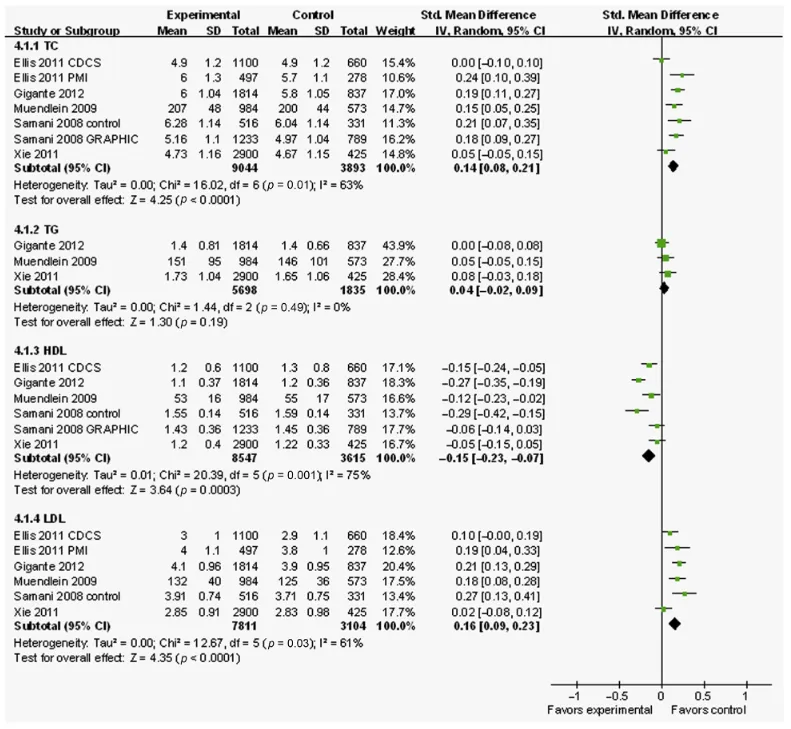
Source: He, Q. C., Hu, Y. Y., Zhang, Q. P., Tan, L. L., Liu, Y. H., Liu, T., ... & Liang, N. (2017). A meta-analysis of three identified single nucleotide polymorphisms at 1p13. 3 and 1q41 and their associations with lipid levels and coronary artery disease. The Kaohsiung Journal of Medical Sciences, 33(1), 1-10.
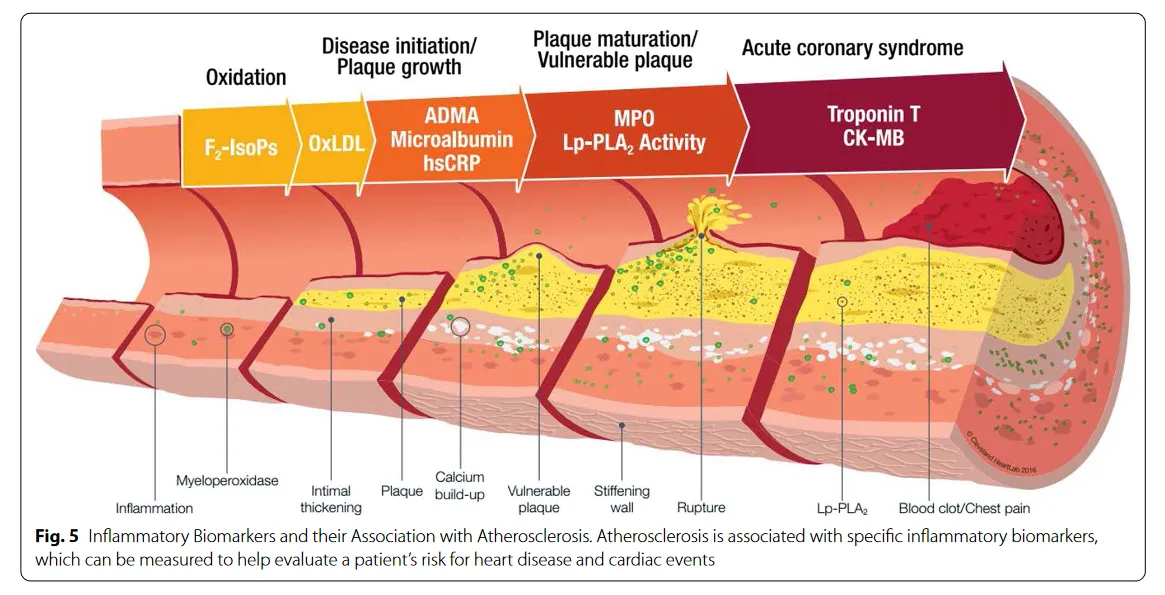
In addition to higher LDL-C levels, the increased risk of CAD in 'A' allele carriers may also be due to higher activity of an enzyme called lipoprotein-associated phospholipase A2 (Lp-PLA2). This enzyme is present on LDL particles and acts to oxidise lipids and promote inflammation. It therefore plays an important role in the formation of fatty plaques.
KEY POINTS
- 'A'-allele carriers have been shown to have a higher risk of coronary artery disease (CAD) compared to those with the GG genotype.
- Increased CAD risk in 'A' allele carriers is likely due to higher LDL cholesterol levels.
- 'A' allele carriers may also have a higher activity of Lp-PLA2: an enzyme that plays a role in the formation of fatty plaques.
Your Protecting your heart (PRSC1) trait
Your Protecting your heart (PRSC1) trait looks at variants of your PRSC1 gene (as well as the closely related SORT1 and CELSR2 genes). Depending on your DNA results, you will be categorised into one of three groups:
- High LDL-C levels and CAD risk - you carry two copies of the risk 'A' allele (rs599839) associated with higher LDL-C levels and a greater risk of CAD.
- Moderately-higher LDL-C levels and CAD risk - you carry one copy of the risk 'A' allele (rs599839) associated with higher LDL-C levels and a greater risk of CAD.
- Average LDL-C levels and CAD risk - you do not carry the risk 'A' allele. Your genotype (GG) is not associated with higher LDL-C levels and CAD risk.
To find out your results, please login to truefeed.