
You eat well. You get outside. You might even supplement. And yet, every time you test your vitamin D levels, the result comes back low.
Sound familiar?
Vitamin D deficiency is one of the most common findings in modern health testing, even among people who are highly health-conscious and regularly active.
So why does it keep happening?
The answer is more interesting - and more personal - than most people realise.
First, Why Vitamin D Levels Matter
Vitamin D isn't just about bones. Low levels are associated with fatigue, low mood, poor muscle function, chronic inflammation, and a weakened immune response.
If you're someone who tracks their health closely, chronically suboptimal vitamin D is the kind of thing that quietly undermines everything else you're trying to do.
What Should I Be Aiming For?
The widely cited target is 50–125 nmol/L. Many people who test regularly are surprised to find themselves below this range, even in summer.
How widespread is this problem? More than you might think. A 2025 analysis of UK adults found roughly half had vitamin D levels below the optimal range - and that's among people actively testing their health. Using the more conservative NHS deficiency threshold, around one in five UK adults is clinically deficient.
Among certain groups the picture is particularly stark: research using UK Biobank data found deficiency rates exceeding 50% in people of Asian ancestry during winter and spring.
The Sunlight Myth You Need to Hear
Here's something that surprises most people: getting outside every day doesn't guarantee adequate vitamin D production.
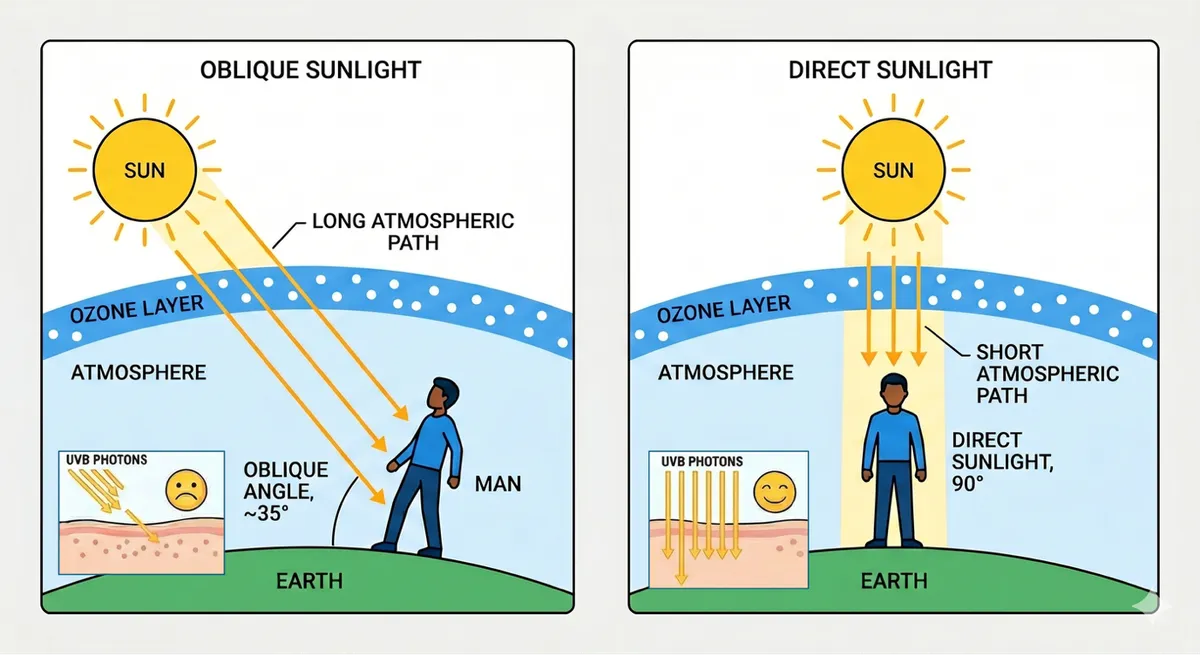
The angle of the sun matters just as much as the amount of time you spend in it. UVB radiation, which is the specific wavelength that triggers vitamin D synthesis in your skin, must travel through the ozone layer to reach you. The more oblique the sun's angle, the more ozone it passes through, and the less UVB arrives at your skin.
What does this mean practically? In the UK, meaningful vitamin D production from sunlight is only possible between roughly late March and September when the sun is at a steep enough angle above the horizon - and even then, only between approximately 10am and 3pm. Your morning walk before work is, unfortunately, delivering very little vitamin D, regardless of how bright it feels.
In winter, this problem becomes even more acute. Between October and March, the sun sits too low in the sky for UVB to reach more northerly latitudes like the UK and North America at meaningful levels at all. You could spend every lunchtime outside and still produce almost nothing.
So if you've been relying on your lifestyle to keep levels topped up, this alone may explain why it has not been as effective as you may have expected.
Why Some People Struggle More Than Others: It’s Biology
Vitamin D doesn't simply arrive in your bloodstream ready to use. It travels a multi-step pathway: produced in the skin, converted in the liver, then activated in the kidneys into its hormonally active form. At each stage, the process depends on enzymes, transport proteins, and cellular receptors, and how well each of those systems function varies from person to person.
That variation is largely genetic.
Small differences in the genes governing vitamin D metabolism can affect how efficiently it's transported through the blood, how readily it's converted into active forms, and how effectively your cells actually respond to it.
The end result is that two people can have identical sun exposure, identical diets, and identical supplement routines - and still show meaningfully different blood test results.
Enter Your DNA
Several key genes influence how efficiently your body produces and processes vitamin D:
GC (Vitamin D Binding Protein) transports vitamin D through your bloodstream to the tissues that need it. Variants in GC are among the strongest genetic predictors of circulating vitamin D levels - stronger, in many studies, than sun exposure or diet alone. If you carry a less efficient variant, vitamin D can be produced perfectly well in your skin but still fail to reach its destination. 7.7% of FitnessGenes members carry a variant associated with reduced transport efficiency.
CYP2R1 controls the critical first conversion step in the liver, turning vitamin D produced in the skin into a usable form. Reduced function here creates a bottleneck before the process has really begun. 23.7% of FitnessGenes members carry a variant associated with impaired conversion at this stage.
VDR (Vitamin D Receptor) is the final piece. Even optimal circulating levels are meaningless if your cells can't respond to them. The VDR gene encodes the receptor that vitamin D must bind to in order to do its job. Certain variants reduce that receptor sensitivity, meaning the same blood level delivers less biological impact. 14.6% of FitnessGenes members carry a variant associated with reduced receptor sensitivity and, consequently, reduced bone mineral density.
If you carry suboptimal variants across several of these genes - which is not uncommon - you may need significantly higher vitamin D levels to achieve the same biological effect as someone with more efficient variants. Standard reference ranges don't account for this. Your "normal" may genuinely need to be higher than someone else's.
Skin Tone Is a Factor Too
Melanin, the pigment that gives skin its colour, provides natural protection against UV radiation. But this protection comes at a cost: it also reduces the skin's ability to synthesise vitamin D. As a result, people with darker skin tones need significantly longer sun exposure to produce equivalent amounts of vitamin D.
Combined with genetic variants affecting conversion and transport, this can create a compounding effect that makes deficiency particularly persistent in those with darker skin tones.
What To Do If Your Vitamin D Is Chronically Low
If testing consistently shows low levels, a few targeted actions are worth considering:
Supplement strategically. For most people in the UK, supplementation during the winter months isn't optional - it's necessary. For those with genetic variants affecting conversion or transport, year-round supplementation is often warranted.
When choosing a supplement, opt for vitamin D3 rather than D2. D3 is the form your body produces naturally from sunlight, is more bioavailable, and raises circulating levels more effectively. A daily dose of 1,000–2,000 IU is a sensible starting point for most people. Those with elevated genetic risk or persistently low test results may need more, but that conversation is best had with a healthcare professional and guided by regular blood testing rather than guesswork.
Take it with fat. Vitamin D is fat-soluble. Taking your supplement with a meal containing healthy fats such as avocado, olive oil, or oily fish, meaningfully improves absorption.
Time your sun exposure. If you're relying on sunlight during warmer months, make it count. Aim for exposure between 10am and 2pm, when UVB is most available. Forearms and legs exposed for 15–20 minutes is more effective than a long walk at 8am with only your face uncovered.
Test, don't guess. Supplementing without testing is flying blind. A simple home blood test, taken every few months, gives you the data to adjust your approach based on your actual levels rather than a generic guideline, and tells you whether what you're doing is actually working.
Know your genetic baseline. Understanding whether you carry variants in GC, CYP2R1, or VDR changes the conversation entirely. It tells you whether you need to be more aggressive with supplementation, and it explains why your levels might not respond the way you'd expect.
A Word on Overdoing It
Recent NHS warnings have flagged a small but real risk of vitamin D toxicity, which is worth putting in context.
Vitamin D toxicity (hypervitaminosis D) occurs when levels in the blood become high enough to cause calcium to accumulate in the body, leading to nausea, weakness, kidney problems and, in severe cases, more serious complications. It is almost always the result of taking very high-dose supplements over a prolonged period. Sun exposure carries no equivalent risk; the body simply stops producing vitamin D once it has enough.
For the vast majority of people in the UK, the far greater risk is having too little, not too much. Around one in five UK adults is clinically deficient. Toxicity from sensible supplementation is rare.
This is exactly why testing matters. The solution to the overdose risk isn't to avoid supplementation, it's to supplement intelligently, with regular testing to keep you in the optimal range.
Know your levels. Adjust accordingly.
The Bottom Line
We’re often told that optimising vitamin D is simple. Get outside. Get some sun. Your body does the rest. And in theory, that’s true. In response to UVB sunlight, your skin synthesises vitamin D3. It’s one of the most elegant biological systems we have.
But the ‘sunlight’ solution isn’t the full story.
Persistently low vitamin D is rarely just a lifestyle problem. For many people, it's the result of genetic variants affecting how efficiently their body produces, converts, transports, and responds to vitamin D - compounded by the practical realities of living in northern latitudes.
Testing your blood levels is a good start, but testing your DNA provides the foundation. It tells you not just where you are, but why you keep ending up there, and what you can actually do about it.
Your genes may not be your destiny. But they are your starting point.
Discover your personal vitamin D genetic profile, along with actionable recommendations tailored to your results, at fitnessgenes.com.
References
1 https://www.forthwithlife.co.uk/blog/uk-vitamin-d-statistics/
2 https://pmc.ncbi.nlm.nih.gov/articles/PMC6561453/
3 https://www.sciencedirect.com/science/article/abs/pii/S0261561420306397