
Why does blood need to clot?
We can think of our circulatory system as similar to the plumbing system in a house. The network of water pipes is akin to our system of blood vessels (i.e. arteries and veins), while the water that is pumped through pipes is analogous to blood.
If one of the pipes were to be damaged (say from an errant drill during an ill-prepared DIY project), a leak could occur. Water would seep out from the pipe, causing the water pressure in the system to drop.
Similarly, damage to blood vessels, such as from a cut or nick, can cause blood to leak out i.e. a bleed. As we all know, one of the main functions of blood is to deliver oxygen, nutrients, hormones, and other important molecules to tissues around the body. Therefore, if bleeding were allowed to proceed unabated, the loss of blood and subsequent drop in blood pressure would impair the delivery of oxygen and nutrients to tissues, compromising their function and eventually leading to death.
If you’re reading this, however, the chances are that you have sustained a cut, nick, blunt trauma, or other form of injury to your blood vessels, but have lived to tell the tale. This is because your blood has the ability to clot or ‘coagulate’, forming a plug that seals gaps in blood vessel walls. Continuing the plumbing analogy, this is equivalent to applying sealant to a hole in a water pipe.
Our blood contains cell fragments, called platelets, that become activated in response to injury to blood vessel walls. These then clump together and form a mesh that patches the injury site. Returning to the plumbing analogy, you may have noticed that sealant also dries and goes hard, to form a robust plug. In the same way, our blood contains various proteins, known as coagulation or clotting factors, that help to create a tough, fibrous substance called fibrin. This supports the formation of a tough, hard blood clot that acts like a band-aid, preventing bleeding and blood loss.
Although clotting (coagulation) is useful for preventing bleeding when blood vessel walls are injured, the process needs to be regulated. Excessive clotting can lead to formation of abnormal blood clots (known as thrombosis) that obstruct blood flow, causing cells and tissues to be starved of oxygen and nutrients.
For this reason, our body has various other anticoagulant molecules that act to inhibit blood clotting and prevent blood clots from becoming too large. We also have enzymes and molecules that act to break down fibrin in blood clots (a process known as fibrinolysis). This process helps to remove blood clots after blood vessel walls are fully repaired, and also prevents blood clots from becoming too large.
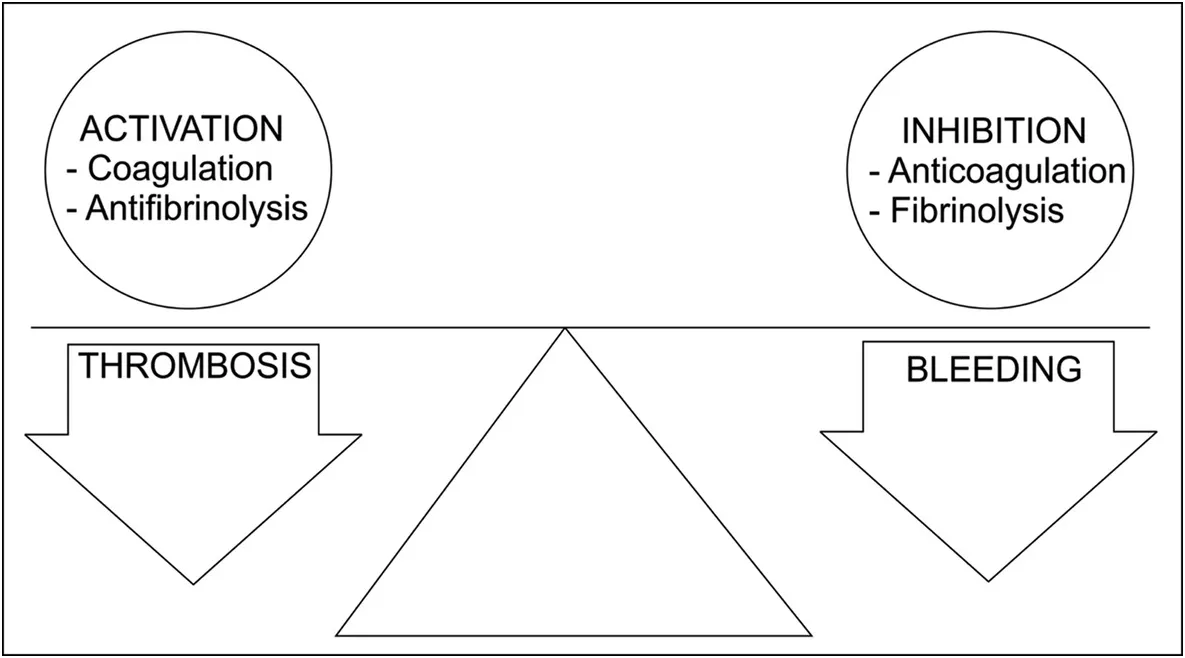
Source: Steurer, M., & Ganter, M. (2017). Coagulation Monitoring of the Bleeding Trauma Patient. In A. Varon & C. Smith (Eds.), Essentials of Trauma Anesthesia (pp. 154-163). Cambridge: Cambridge University Press. doi:10.1017/9781316874936.012
These anti-coagulant / fibrinolytic processes, however, also need to be kept in check. If there is excessive inhibition of blood clotting, injuries to blood vessel walls will not be sealed, making us more susceptible to bleeding.
Our bodies therefore need to maintain a careful balance between clotting (coagulation) and anti-coagulation. As we’ll find out in this trait, changes in the activity of various pro- and anti-coagulant proteins can affect our risk of developing abnormal blood clots or excessive bleeding.
How does blood clot?
The process by which a blood clot forms (coagulation) is complex and involves the walls of blood vessels, platelets, coagulation (or clotting) factors, and various other enzymes and signalling molecules.
To simplify things slightly, we can split blood clotting into the following stages:
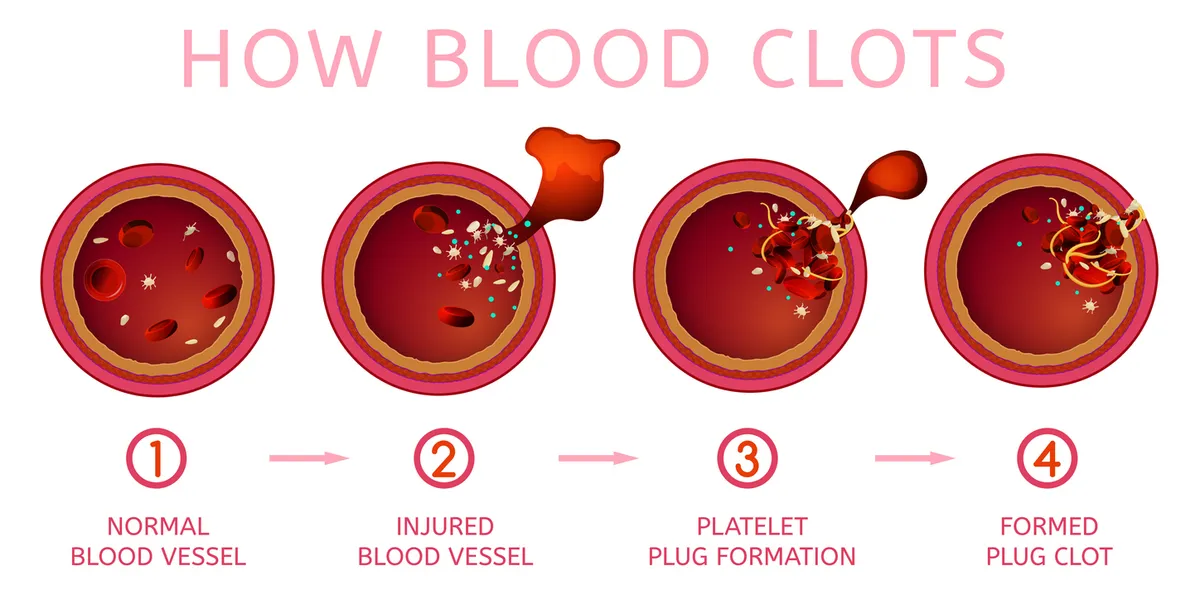
- Sustaining damage to a blood vessel wall.
- Formation of a “platelet plug”
- Activation of a coagulation cascade resulting in the production of fibrin.
- Cessation of clotting once an adequate blood clot is formed.
Let’s take a quick look at each of these stages individually.
Damage to a blood vessel wall
Given that platelets and coagulation factors are freely circulating in the bloodstream, you may ask why don’t they spontaneously form blood clots? The reason is because the inner lining of blood vessels that is direct contact with flowing blood (called the endothelium) produces various molecules that prevent clotting/coagulation.
By contrast, the layer underneath the endothelium (subendothelium) produces molecules that promote blood clotting.
In the event of injury to a blood vessel wall, such as from a cut, blunt trauma, damage caused by turbulent blood flow, or damage from oxidised lipids in the bloodstream, this subendothelial layer gets exposed to blood.
This stimulates vasoconstriction (narrowing of blood vessels) and the release of chemicals that cause platelets to migrate and stick to the blood vessel wall at the injury site.

Formation of a platelet plug
Platelets that stick to the blood vessel wall at the injury site become ‘activated’ by binding to collagen and a substance called von Willebrand factor in the subendothelium. Activation of platelets causes them to change their shape: they become more irregular and spiky to increase surface area, allowing them to clump together more effectively.
Activated platelets also release molecules that activate and attract other platelets to the injury site. This leads to the formation of what is a known as a primary platelet plug that seals the injury site and prevents bleeding.
Activation of coagulation cascade
Although the primary platelet plug does a decent job of patching up a leak and preventing bleeding, it needs to harden and become a robust, stable blood clot. This is where coagulation factors (or clotting factors) come in.
Coagulation factors are essentially inactive enzymes, mainly produced by the liver, that circulate in the bloodstream. They are numbered I – XIII, in order by which they were discovered. In response to injury to the blood vessel wall, coagulation factors serially activate one another in a complex series of reactions known as the coagulation cascade.
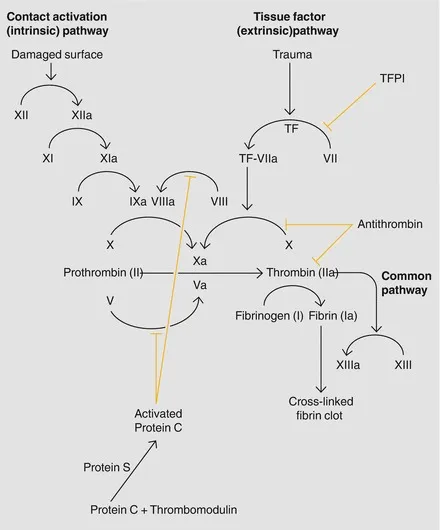
Source: Shantsila E, Lip GYH. Non-Vitamin K Antagonist Oral Anticoagulants: A Concise Guide [Internet]. Cham (CH): Adis; 2016. Figure 1.1, [The coagulation cascade]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK500197
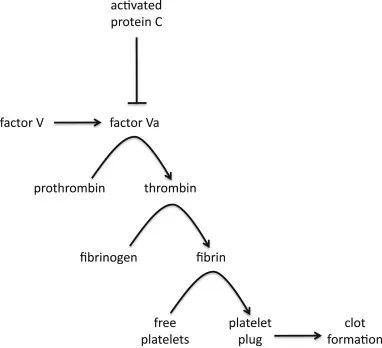
The result of this cascade is to convert an inactive coagulation factor called prothrombin (or Factor II), into its active form, thrombin (Factor IIa). Thrombin then produces the tough, insoluble, fibrous substance called fibrin (Factor Ia) from its precursor, fibrinogen (Factor I). It is strands of fibrin produced on the surface of platelets that add stability to the blood clot.
Individual fibrin molecules join with one another to form a larger fibrin strand (polymer). Fibrin strands then form cross-links with one another to create a robust mesh or scaffold that strengthens the blood clot, traps more platelets, and forms a rigid plug that prevents bleeding.
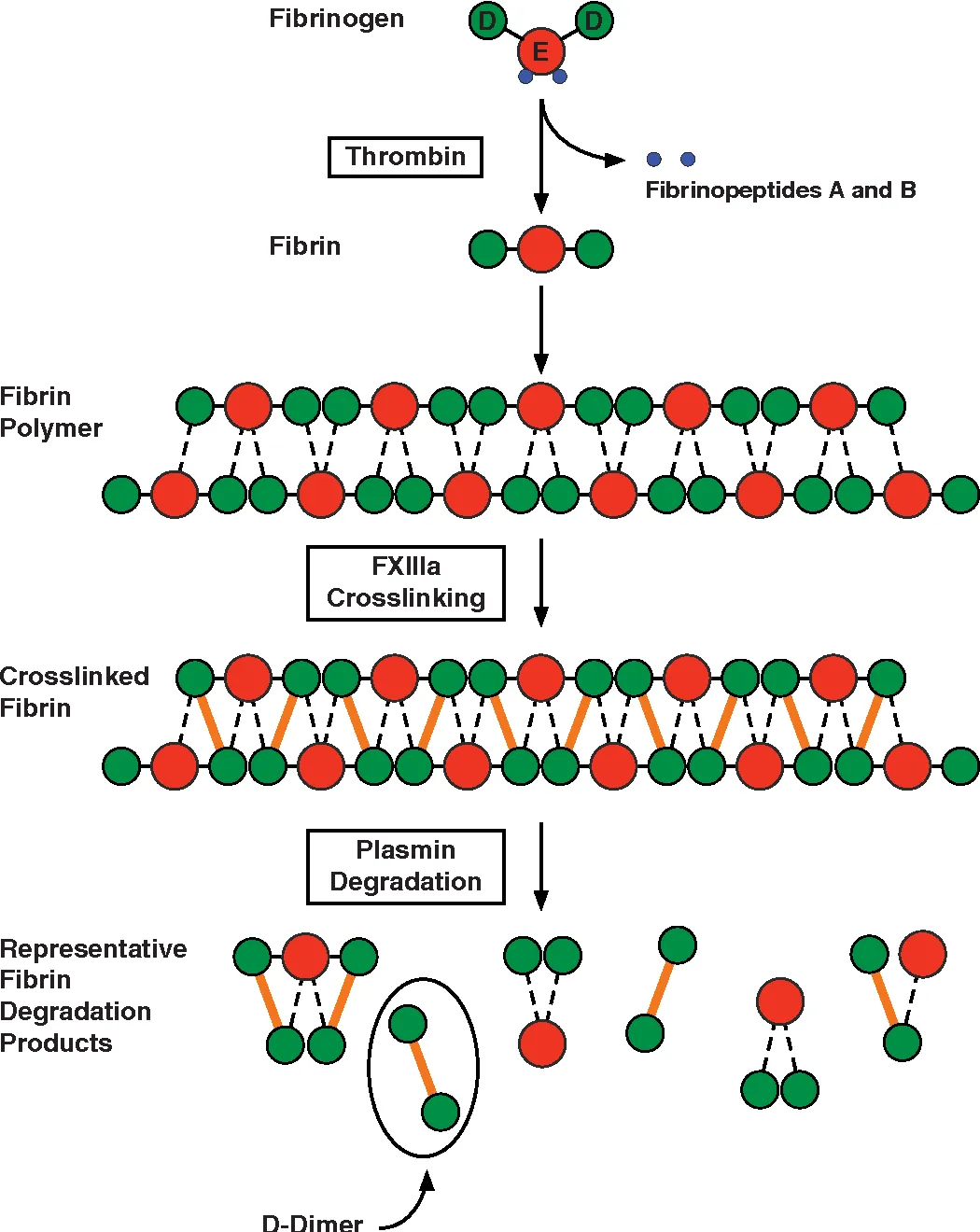
Source: Riley, R.S., Gilbert, A.R., Dalton, J.B., Pai, S.S., & Mcpherson, R.A. (2016). Fibrinogen Thrombin FXIIIa Crosslinking Plasmin Degradation Fibrinopeptides A and B Fibrin Polymer Crosslinked Fibrin Representative Fibrin Degradation Products Fibrin.
Cessation of blood clotting
If the blood clotting process were allowed to continue unabated, the ensuing blood clot would become excessively large, obstructing blood flow through the blood vessel. We have therefore have various anticoagulant molecules that inhibit coagulation factors, thereby preventing blood clots from becoming larger than necessary.
For example, we produce an anticoagulant molecule called antithrombin, which inhibits thrombin (Factor IIa), thereby preventing the production of fibrin strands. Another important anticoagulant is called activated protein C. This inhibits coagulation factors V and VIII in the coagulation cascade, ultimately preventing the formation of fibrin in blood clots.
In addition to anticoagulant molecules that inhibit clotting, we also have various enzymes (e.g. plasmin) that actively dissolve fibrin and shrink blood clots. This process is known as fibrinolysis and it helps to both prevent blood clots from becoming too large and shrink existing blood clots after blood vessel wall injuries are healed. This ensures blood can still flow unobstructed through blood vessels.
What is Factor V?
Factor V is a coagulation factor that helps to form blood clots. It is coded for by the F5 gene.
As described in the previous section, in response to injury to a blood vessel wall, a series of chemical reactions, known as the coagulation cascade, serves to produce a tough, fibrous substance called fibrin. Strands of fibrin form a mesh that traps platelets at the injury site and creates a strong, stable clot that prevents blood loss.
Factor V (or, more accurately, its active form Factor Va) assists with one particular stage of the coagulation cascade: it converts prothrombin (Factor II) into thrombin (Factor IIa). In turn, thrombin then converts fibrinogen, which is dissolved and circulating in the bloodstream, into fibrin, the tough, insoluble material that stabilises blood clots.
Source: LaBonte, M. L. (2014). Anticoagulant factor V: factors affecting the integration of novel scientific discoveries into the broader framework. Studies in History and Philosophy of Science Part C: Studies in History and Philosophy of Biological and Biomedical Sciences, 47, 23-34.
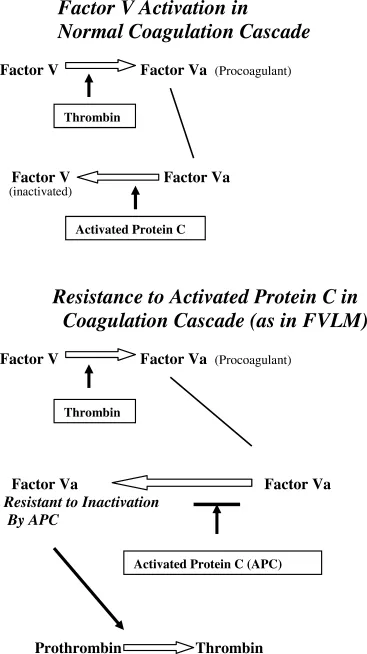
Factor V (or, more accurately, its activated form, Factor Va) is inhibited by an anticoagulant protein called activated protein C (APC). By inhibiting or deactivating factor Va, APC serves to slow the production of fibrin and prevent a blood clot from becoming larger than required.
As we’ll elaborate on in the following section, some people produce an abnormal version of Factor V that is harder to deactivate. This can lead to excessive clotting and increase the risk of forming of abnormal blood clots.
What is Factor V Leiden?
Factor V Leiden is an inherited disorder that makes blood more likely to clot.
It is caused by a mutation, known as the Leiden mutation, in the F5 (Factor V) gene. People who inherit this mutation produce an abnormal form of the Factor V coagulation factor, called Factor V Leiden.
Unlike normal Factor V, the abnormal Leiden form of Factor V is difficult to inactivate. As explained in the previous section, an anticoagulant molecule called activated protein C (APC) serves to inhibit or deactivate Factor Va (the active form of Factor V), thereby switching off the production of thrombin. This, in turn, prevents the production of fibrin and the formation of a blood clot.
Source: Cohen, S. M. (2004). Factor V Leiden mutation in pregnancy. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 33(3), 348-353.
By contrast, Factor V Leiden has an abnormal shape, making it more difficult for APC to bind to and deactivate (a phenomenon also referred to as APC resistance). As a result, people who inherit the Leiden mutation and produce Factor V Leiden turn off blood clotting (coagulation) much more slowly. (On this note, studies suggest the Leiden variant is deactivated 10x more slowly compared to the normal Factor Va). This can increase the risk of developing abnormal blood clots.
In particular, people with Factor V Leiden are several times more likely to develop abnormal blood clots in their veins (venous thromboembolism), such as in deep veins in the limbs (deep vein thrombosis).
How do genes cause Factor V Leiden?
Factor V Leiden is caused by the Leiden mutation in the F5 (Factor V) gene.
This mutation, also designated rs6025, causes a G>A change in the DNA code of the F5 gene. This results in an amino acid substitution (R506Q) in the amino acid sequence of the Factor V protein, with arginine being replaced by glutamine. As mentioned earlier, this abnormal version of the Factor V protein is a different amino acid sequence is more difficult to inactivate, making it harder to switch off blood clotting.
As we inherit pairs of every gene (one from our mother, the other from our father), it is possible to inherit either one or two copies of the Leiden mutation / Leiden variant of the F5 gene.
People who inherit one copy of the mutation are said to be heterozygous Factor V Leiden. This means they have one copy of the normal F5 gene and one copy of the Leiden F5 variant. Consequently, roughly 50% of the Factor V coagulation factor/protein produced by people with heterozygous Factor V Leiden is the abnormal Leiden form.
Individuals with homozygous Factor V Leiden have inherited two copies of the Leiden mutation, meaning both copies of their F5 gene are the abnormal Leiden variant. This results in 100% of the Factor V produced being the abnormal Leiden form. Unsurprisingly, those with homozygous Factor V Leiden switch blood clotting more slowly than those with heterozygous Factor V Leiden, which engenders a much higher risk of developing abnormal blood clots.
How common is Factor V Leiden?
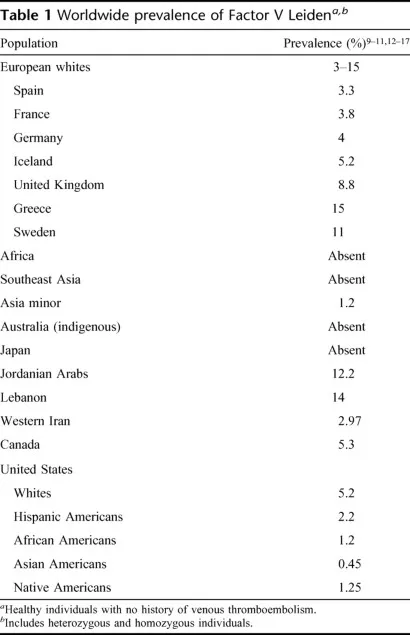
It is estimated that about 3-8% of European and US populations are heterozygous Factor V Leiden. By contrast, homozygous Factor V Leiden is extremely rare, occurring in less than 1% of populations. About 1 in 5000 people from white populations have homozygous Factor V Leiden.
Source: Kujovich, J. L. (2011). Factor v Leiden thrombophilia. Genetics in Medicine, 13(1), 1-16.
As illustrated in the table above, the prevalence of the Leiden mutation varies considerably between various ethnic populations.
On this note, the Leiden mutation is much rarer in African, Asian, and indigenous Australian populations. This thought to be due to the Leiden mutation arising about 20,000 – 30,0000 years ago in the human genome, after Asian, African, and indigenous Australian populations had separated from white populations in the evolutionary timeline.
What is venous thromboembolism (VTE)?
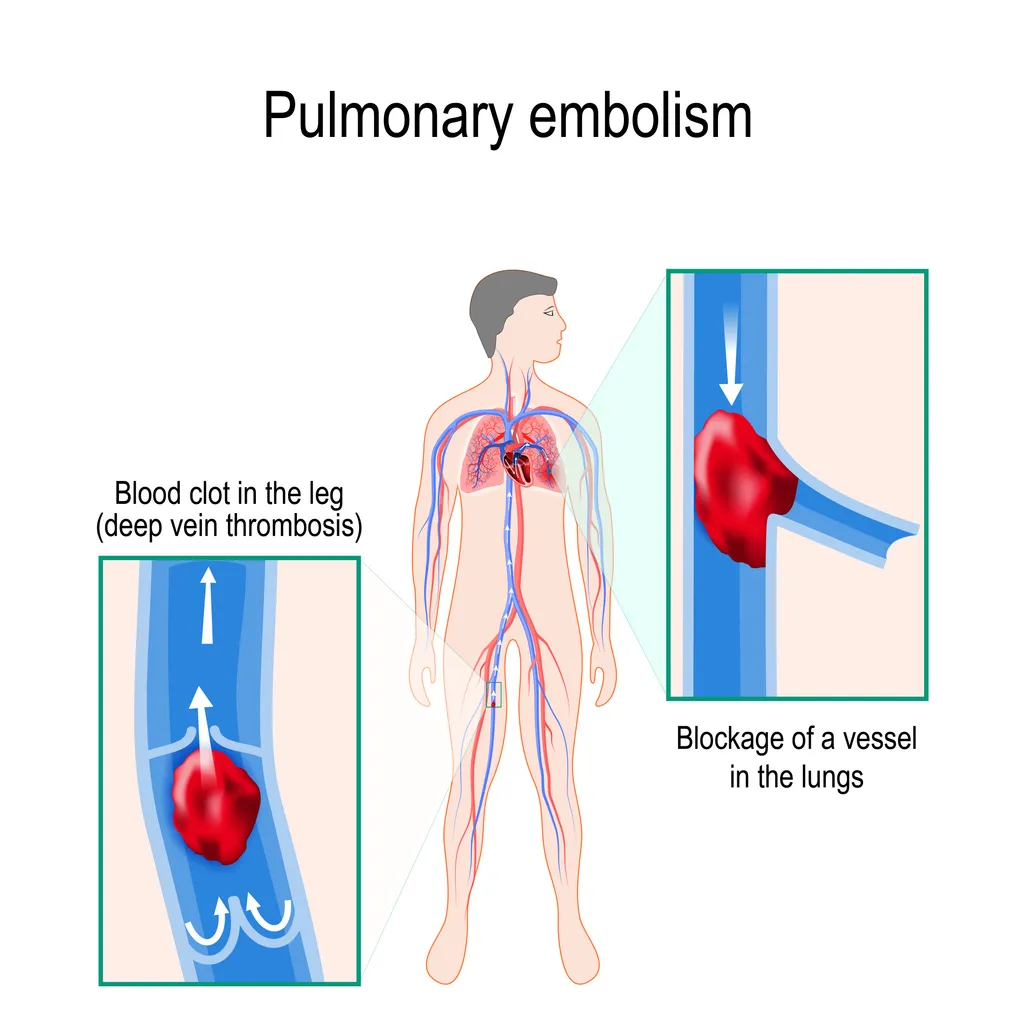
Venous thromboembolism (VTE) describes the formation of abnormal blood clots (thrombi (singular = thrombus)) in veins. Sometimes, pieces of blood clots can break off, travel in the bloodstream, and become lodged at another site in the venous system. This is known as an embolus.
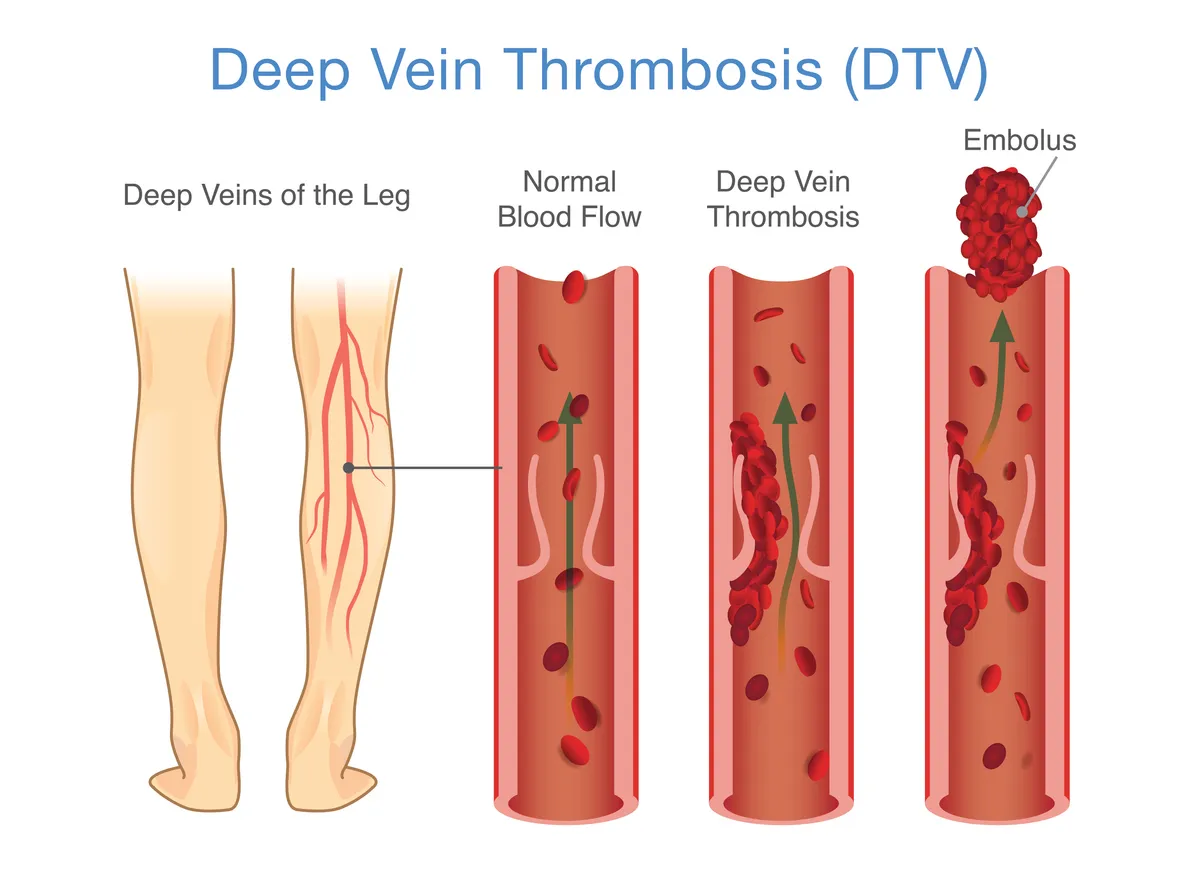
Blood clots are more likely to form in deep veins of the body, particularly in those carrying blood away from the legs. When this occurs, it is referred to as deep vein thrombosis (DVT).
As the blood clot obstructs the flow of blood back to the heart, it causes a build-up of pressure in the vein, leading to swelling, a throbbing or cramping pain, and warmness to touch. Many people with a DVT, however, experience no symptoms at all.
In many cases, a DVT can break off and form an embolus, which is carried to right side of the heart and then becomes lodged in the pulmonary arteries supplying the lungs. This is known as a pulmonary embolism (PE).
A pulmonary embolism is a medical emergency, as blocking an artery to the lung can result in the death of lung tissue, causing the inadequate oxygenation of blood.
The term venous thromboembolism (VTE) covers both DVT and pulmonary embolism (PE), either co-occurring together or separately, as well as blood clots in other veins.
Approximately 1 in every 1,000 people develop a DVT or PE each year, although this figure varies considerably by age, with older people at much greater risk. For people in their twenties, roughly 1 in 10,000 can expect to develop a DVT/PE per year. For those in their seventies, about 5 in every 1,000 people will develop a DVT/PE each year.
People with disorders that make their blood more likely to clot (e.g. those with Factor V Leiden) have a greater risk of developing a DVT or PE.
How does Factor V Leiden increase the risk of VTE?
People with Factor V Leiden are at greater risk of venous thromboembolism (VTE) and developing deep vein thrombosis (DVT), with or without a pulmonary embolism (PE).
The underlying reason for this is fairly easy to follow. As the abnormal Leiden form of Factor V is harder to inactivate, causing clotting to be switched off more slowly, people with Factor V Leiden are more susceptible to developing abnormal blood clots, particularly in their venous system.
The magnitude by which the risk of VTE is elevated depends on whether a person is heterozygous Factor V Leiden (i.e. with one copy of the Leiden mutation) or homozygous Factor V Leiden (i.e. with two copies of the Leiden mutation).
Heterozygous Factor V Leiden
A review of the evidence suggests that those with heterozygous Factor V Leiden have a 3-8 times greater risk of VTE. For example, a 2013 meta-analysis found that those carrying one copy of the Leiden mutation had a 4.38 times higher odds of having VTE compared to those without the mutation. This is illustrated in the Forest plot below.
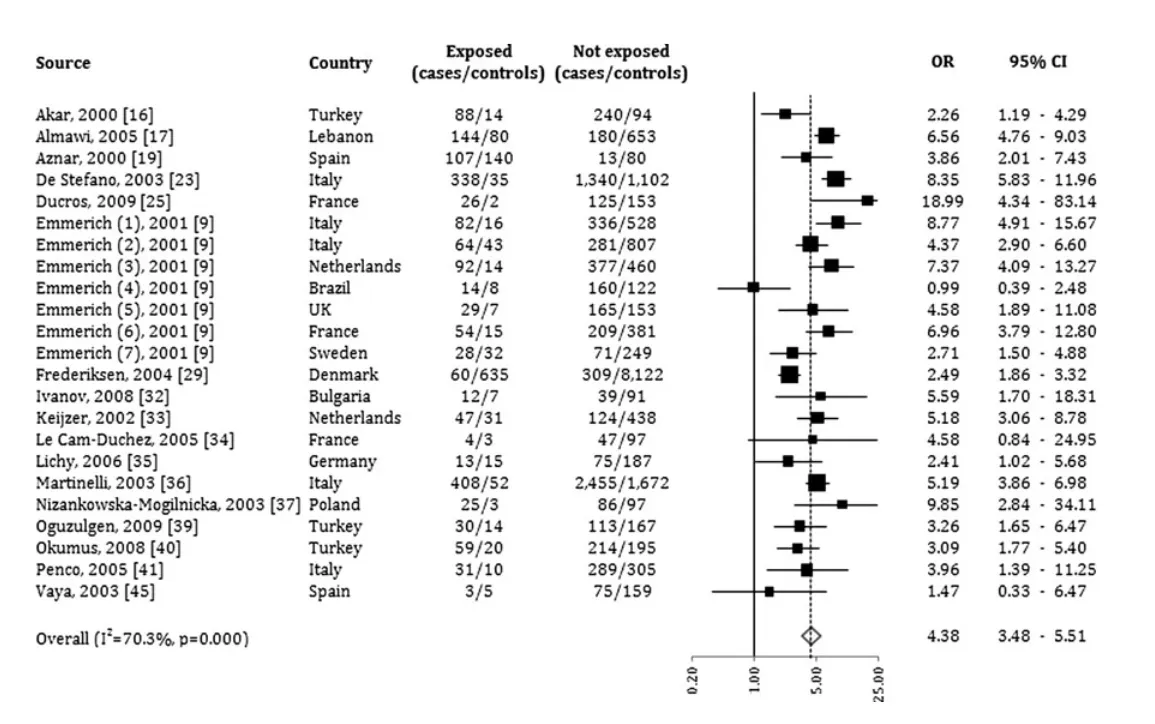
Source: Simone, B., De Stefano, V., Leoncini, E., Zacho, J., Martinelli, I., Emmerich, J., ... & Boccia, S. (2013). Risk of venous thromboembolism associated with single and combined effects of Factor V Leiden, Prothrombin 20210A and Methylenetethraydrofolate reductase C677T: a meta-analysis involving over 11,000 cases and 21,000 controls. European journal of epidemiology, 28(8), 621-647.
Given that roughly 1 in every 1,000 people develop VTE each year, a 3-8 times higher relative risk in those with heterozygous Factor V Leiden corresponds to an absolute risk of 3-8 in every 1,000 people developing VTE each year. This can still be considered to be low.
Similarly, another 2011 study estimated that about 0.5% of people with heterozygous Factor V Leiden develop VTE each year. Another study suggested the lifetime risk of having a VTE in such individuals is 10% or less.
Homozygous Factor V Leiden
Individuals with homozygous Factor V Leiden are at a much greater risk of developing VTE.
A review of the evidence suggested that homozygotes have a 9 to 80 times greater risk of VTE. On this note, a 2013 meta-analysis found that those with homozygous Factor V Leiden had a 11.45 times greater odds of VTE compared to those without the Leiden mutation.
This increase in relative risk of VTE corresponds to an absolute risk of between 9 and 80 people in every 1,000 with homozygous Factor V Leiden developing a DVT, PE, or other form of VTE each year.
Other lifestyle factors can further amplify the risk of VTE in those with the Leiden mutation. These include: taking the combined oral contraceptive pill, taking oral hormone replacement therapy (HRT), being overweight or obese, and sustaining a minor leg injury.